
ADHD and Menstrual Cycle: Why Symptoms Shift

There's a pattern in the ADHD and menstrual cycle relationship that comes up frequently in clinical care and doesn't get nearly enough attention. Women who are reasonably well-managed on their medication for most of the month hit a predictable rough patch in the days before their period: focus drops, executive function gets harder, sleep becomes worse, and the medication doesn't seem to be working as well. Most of the time, this gets written off as PMS and nothing more is made of it. What research has been making increasingly clear is that the connection is real, it has a specific biological explanation, and understanding it changes how ADHD should be treated. For women in Portland, Oregon and across the state, it's a pattern worth naming correctly.
Why Estrogen Has More to Do With ADHD Than Most People Know
Estrogen does a lot of work in the brain beyond its reproductive role. One of those jobs is supporting dopamine, the neurotransmitter at the center of how ADHD works. Estrogen helps the brain produce dopamine, keeps it active between nerve cells, and slows down how quickly it gets broken down. When estrogen is up, dopamine tends to run better. When estrogen falls, it takes some of that dopamine activity with it.
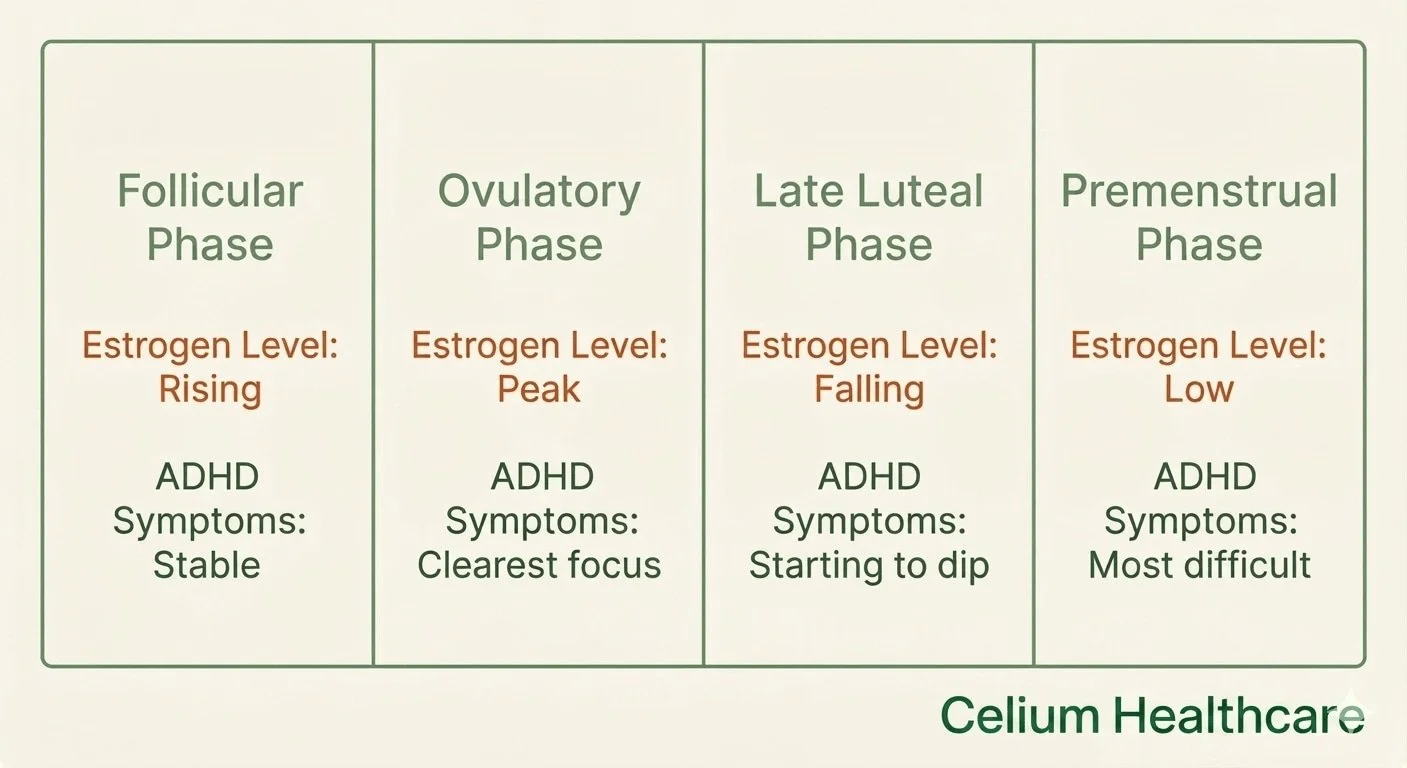
During the first half of the menstrual cycle, called the follicular phase, estrogen rises toward its peak at ovulation. Dopamine is functioning closer to optimal. For many women with ADHD, this is when things feel most stable: tasks get done, focus holds, and medication works the way it usually does.
After ovulation, estrogen starts coming down. In the ten days or so before your period (the late luteal phase), it reaches its lowest point in the cycle, and dopamine drops with it. For someone with ADHD, who is already working from a lower dopamine baseline, that hormonal dip hits harder than it would for someone without the condition.
A 2025 review of 29 studies published in the Journal of Clinical Medicine found that hormonal changes across the menstrual cycle measurably affect attention, working memory, and impulse control, with the strongest effects in women with ADHD.
What the ADHD and Menstrual Cycle Pattern Looks Like
The rhythm is predictable once you start paying attention to it. The two weeks after your period tend to feel more stable: tasks are easier to start, focus holds better, and emotional reactions feel proportionate to what's actually happening. Around ovulation, many women are at their sharpest.
Then the shift happens.
In the week or two before menstruation, staying focused takes real effort. Starting things that require mental energy becomes a bigger ask than usual. Things that didn't bother you much a week ago start to get under your skin. Emotional reactions come faster and take longer to settle. Sleep often gets worse, which makes everything else harder on top of that.
Women who start tracking the ADHD and menstrual cycle pattern often see this emerge very clearly on a calendar. Many spend years assuming it's just part of who they are before a period, never connecting it to ADHD at all.
Research published in Psychoneuroendocrinology found that ADHD symptoms, particularly inattention, tracked directly with reproductive hormone levels across the cycle. That's not random mood variation. It follows the estrogen curve.
Why Your ADHD Medication Can Feel Weaker Before Your Period
This is one of the most practically important parts of the ADHD and menstrual cycle relationship to understand. Stimulant medications work by increasing dopamine availability in the brain. That's how they improve focus, reduce impulsivity, and make it easier to manage tasks and decisions.
But in the late luteal phase, when estrogen has already pulled dopamine down, the medication is working against a smaller supply. The dose hasn't changed. The drug is doing exactly what it normally does. What changed is the hormonal environment it's working in, and that environment makes the same dose less effective than it was two weeks earlier.
A lot of women interpret this as their medication stopping working, or assume they need a permanently higher dose. In most cases, the better explanation is that dopamine levels shift predictably with the cycle, and a fixed daily dose doesn't account for that monthly dip. This is a pharmacological reality, not just a subjective feeling, and it's worth raising with a prescriber when it keeps happening month after month.
A 2025 expert consensus paper in Frontiers in Global Women's Health concluded that hormonal shifts throughout the female lifespan worsen ADHD symptoms, and that medication strategies tailored specifically for women remain an underdeveloped area of care. You can see how this kind of evaluation fits into a broader workup on Celium Healthcare's ADHD services page.
PME vs. PMDD: Two Different Problems That Look Similar
Premenstrual Exacerbation (PME) of ADHD and Premenstrual Dysphoric Disorder (PMDD) are not the same condition. They can look very similar, and they get mixed up regularly, including in clinical settings.
PMDD is its own disorder. Symptoms appear in the late luteal phase and go away completely after menstruation. The defining feature is a genuinely symptom-free window during the follicular phase every cycle. PMDD is primarily related to serotonin and GABA activity, and treatment typically involves SSRIs or certain hormonal contraceptives.
PME of ADHD looks different. ADHD doesn't go away after your period. Symptoms are present throughout the cycle, peak premenstrually, and then settle back to the person's regular baseline after menstruation starts. Not to zero. Back to baseline. The underlying mechanism is dopaminergic, and PMDD treatments tend to miss it entirely because they're aimed at a different system.
A 2021 study by Dorani and colleagues found that women with ADHD are significantly more likely to show hormone-related mood symptoms that look like PMDD. In some of those cases, what's actually happening is that undertreated ADHD is intensifying premenstrually, rather than a separate cyclical mood disorder developing. Tracking symptoms across both phases of at least two full cycles is the most reliable starting point for telling the two apart.
What to Track Before Your Next Appointment
The most targeted data on this topic comes from a 2023 case series by de Jong and colleagues, published in Frontiers in Psychiatry. Nine women with ADHD, several of whom also had PMDD, tried a temporary increase in their stimulant dose during the premenstrual week, roughly 30 percent above their usual dose and only during those specific days. All nine reported meaningful improvements in both ADHD and mood symptoms. Side effects were minimal. Every participant chose to keep doing it over a follow-up period of six to twenty-four months.
This is a small sample and still early data. But the logic is sound, and it's the most directly targeted pharmacotherapy evidence available for this specific pattern.
For women in Oregon managing a predictable monthly drop in how well their treatment works, the most useful thing to bring to an appointment is concrete documentation. Two months of daily symptom notes organized by cycle phase, rather than a general sense that things get harder before a period, gives a prescriber something real to work with. That kind of tracking can meaningfully shift how the ADHD and menstrual cycle pattern gets addressed in your care.
Erik Lee, PMHNP-BC, is a board-certified psychiatric nurse practitioner at Celium Healthcare in Portland, Oregon, with focused training in ADHD evaluation and medication management for adults. If there's a consistent monthly pattern in your symptoms that your current treatment doesn't fully address, a psychiatric evaluation can help determine whether a different approach makes sense.
To schedule a visit, book an appointment online or call (888) 9-CELIUM (923-5486). Visit the rates and insurance page to check your coverage.
Common Questions
-
The ADHD and menstrual cycle connection comes down to estrogen. When estrogen drops in the late luteal phase (the week or two before your period), dopamine levels tend to fall with it. ADHD already involves a lower dopamine baseline, so that hormonal dip hits harder. The result is more difficulty concentrating, worse emotional regulation, and harder executive function in the premenstrual window.
-
For many women, it does, and there's a real reason behind it. Stimulants increase dopamine availability, but when estrogen has already lowered dopamine levels in the late luteal phase, the medication is working against a smaller supply. The dose hasn't changed. What changed is the hormonal environment. This is a monthly, predictable shift, not a sign the medication has permanently stopped working.
-
They're related but different. PMDD, the most severe form of PMS, involves symptoms that fully clear up after menstruation, with a genuinely symptom-free window each cycle. Premenstrual exacerbation of ADHD doesn't work that way. Symptoms return to baseline after your period, not to zero. One is primarily serotonin-driven, the other dopamine-driven. Tracking symptoms across both phases is the most reliable way to tell them apart.
-
[1] de Jong, M., Wynchank, D. S. M. R., van Andel, E., Beekman, A. T. F., & Kooij, J. J. S. "Female-specific pharmacotherapy in ADHD: Premenstrual adjustment of psychostimulant dosage." Frontiers in Psychiatry. 2023. https://doi.org/10.3389/fpsyt.2023.1306194
[2] Dorani, F., Bijlenga, D., Beekman, A. T. F., van Someren, E. J. W., & Kooij, J. J. S. "Prevalence of hormone-related mood disorder symptoms in women with ADHD." Journal of Psychiatric Research. 2021. https://doi.org/10.1016/j.jpsychires.2020.12.005
[3] Roberts, B., Eisenlohr-Moul, T., & Martel, M. M. "Reproductive steroids and ADHD symptoms across the menstrual cycle." Psychoneuroendocrinology. 2018. https://doi.org/10.1016/j.psyneuen.2017.11.015
[4] Wynchank, D., Sutrisno, R. M. G. T. M. F., van Andel, E., & Kooij, J. J. S. "Menstrual Cycle-Related Hormonal Fluctuations in ADHD: Effect on Cognitive Functioning, A Narrative Review." Journal of Clinical Medicine. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12786913/
[5] Kooij, J. J. S., de Jong, M., Agnew-Blais, J., et al. "Research advances and future directions in female ADHD: the lifelong interplay of hormonal fluctuations with mood, cognition, and disease." Frontiers in Global Women's Health. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12277363/
[6] Wynchank, D., de Jong, M., & Kooij, J. J. S. "Practical tools for female-specific ADHD: The impact of hormonal fluctuations in clinical practice and from the literature." European Psychiatry. 2025. https://doi.org/10.1192/j.eurpsy.2025.10120
This post is for informational purposes only and does not constitute medical advice or establish a patient-provider relationship. Always consult a qualified healthcare provider about your specific situation. If you are in crisis, call 911 or text/call 988.
Clinically supervised by Erik Lee, PMHNP-BC | Celium Healthcare | celiumhealthcare.com